
A new chance for interventional MR?
October 25, 2017
By Michael Friebe
The unparalleled soft tissue contrast and excellent image quality of MR have made it the imaging modality of choice especially for neuro and oncological applications.
The obtained MR images are then frequently used as relevant preoperative images for surgery planning, or as a visual reference directly in the surgery suite.
MR systems directly employed for therapeutic guidance or surgical monitoring are rarely available. The standard imaging systems in the surgery room are typically X-ray, ultrasound or endoscopy (video) performing the patient monitoring, controlling and device guiding functions.
Figure 1 (click image in upper right corner): Typical horizontal field 3T system with 70cm bore diameter. Actual therapy is difficult for the surgeon and only very little vertical space is available. A holding arm could be very helpful (shown in black), but must be very small and flexible to be of use.
To use these preoperative MR images also for therapy purposes usually requires fusion with the available imaging data in the surgery room. That is either not done, or happens only in the head of the clinician, so called cognitive fusion, or is accomplished by more or less accurate and complicated special software tools in combination with optical and/or electromagnetic device tracking systems.
For this fusion via software-based image co-registration the images are manually or semi-automatically registered to each other. A preoperative MR image, as the wording implies, was taken before the surgery, however, sometimes even on a bed with different curvature than the surgery table or in a different patient position.
For prostate MR, for example, the imaging is typically done with the patient in a straight supine position, while the actual biopsy or therapeutic treatment is performed prone or supine with the legs angled toward the torso. And for breast MR, the patient typically lies in an elevated prone position while surgery is performed on a surgical table in supine position or on the side. You easily recognize the difficulties using these preoperative MR images for accurate image fusion with the available imaging modalities available in the therapy or surgery room.
Real, precise registration is not possible that way with typical image registration errors in the order of 3-7mm, and in case of missing fiducial marker structures sometimes even significantly larger. That may be sufficient for actual therapies using an additional imaging system or for coarse orientation, but is too large for tissue biopsies and other precise therapies on small structures.
Using real time MR as a guidance device for intraoperative or interventional therapies (eg. biopsies and treatment of prostate cancer, liver laser-/radio-frequency-/ or cryo-ablations, brain interventions) could be very beneficial and would obviously eliminate or greatly reduce these registration errors.
This requires, however, that the therapeutic procedure is performed in the MR suite or the MR system is placed in a dedicated surgery room. The latter is an option that is explored by several institutions, but comes with very high investments and very highly skilled interdisciplinary staff.
Difficult patient access in conventional horizontal field superconductive magnets, and the need for special non-ferromagnetic therapy tools have also prevented a widespread occasional interventional use of conventional diagnostic MR systems. The interventional and therapeutic use of MR follows for the last 20-plus years the strategy to employ conventional standard high-field systems and add more or less complicated and expensive components.
MR-compatible robotic systems were, for example, proposed to solve the patient access issue in combination with specially shielded in-room monitors, dedicated nitinol or plastic devices with no or little susceptibility-related imaging artifacts, and in-room optical tracking systems. These components are quite expensive and the possible therapies are still limited because of the tight space in the MR bore and the issues around surgical sterility. The robotic systems are even needed with the short-bore magnets of the newest MR generation. With a magnet length of 1.2 meters it is still 60cm (an arms length) to the center of the magnet and with a bore diameter of 70cm, with a mid-size patient placed, there is only 10-15cm of available vertical space for a therapy tool (see figure 1).
Open vertical field magnets do provide some benefits for interventional procedures, but typically have only magnetic field strength of 0.2T to 0.4T with currently only one system over 1T. Lower field strength comes with increased acquisition times, which is not good for therapy applications, and a lower image quality. On the other hand, the lower field strength also reduces susceptibility artifacts and comes with a much lower magnetic attraction force, making the surgery generally safer.

Figure 2: A tablet ultrasound of a large diagnostic imaging vendor placed only 1m away from the 3T MRI of another large imaging vendor. The ultrasound system is not approved and certified for use in the MRI suite, but direct applications under ultrasound guidance could give a new boost to performing interventional and therapeutic procedures in the MRI suite under ultrasound guidance. The picture on the right shows the cognitive fusion of MRI and US images on separate monitors.
So why not use the MR imaging capabilities and continue the procedure inside the imaging suite with an ultrasound system that is either cognitively fused (see figure 2) or automatically co-registered and overlaid to the just obtained MR images. Several commercially available ultrasound systems could theoretically be used even up to 1m to a 3T magnet opening (see figure 2). While these systems do not have an official MR safe label, research institutions have used these systems in phantom set-ups to rethink interventional MR procedures.
First, a comprehensive MR scan could be performed and the patient moved out of the magnet bore, but remaining on the MR bed. Live ultrasound images that are tracked using an optical inside-out approach adding a camera to the ultrasound probe in combination with an optical reference marker are then immediately fused with the MR images (see figure 3). This allows a comfortable US guided intervention and excellent patient access directly on the MR patient bed. This could then be combined with partly 3-D printed entirely mechanical MR compatible 7DOF holding arms keeping therapy devices and other tools in place (see figure 1). If additional MR imaging is required, the patient is moved back in the MR system. This set-up creates a very cost-efficient and effective environment that combines the advantages of MR and US by largely avoiding the drawbacks. And since most MR systems are almost exclusively used for diagnostic purposes, such an easy to set up and remove system would even be attractive for sites that only do few interventional or therapeutic MR procedures.

Figure 3: The concept of combining MR images directly with ultrasound inside the MR suite. For that, markers on the patient are used and a small camera system that is directly mounted to the ultrasound probe. The live ultrasound is then registered to the MR image and the actual procedure performed under ultrasound guidance. If additional MR imaging is required, then the patient is moved back into the magnet bore and subsequently the ultrasound registered again to the new image data set.
MR/ultrasound fusion is already offered by several vendors for prostate biopsy applications. With MR-compatible and approved ultrasound systems and easy-to-use and inexpensive accessories, interventional MR could become an attractive option again, also for other clinical applications.

About the author: About the author: Professor Michael Friebe, Ph.D., has been involved in diagnostic imaging and imageguided therapeutic products and services, as founder/ innovator/CEO, investor and scientist. Dr. Friebe is a board member of three startup R&D companies, as well as the investment partner of a medical technology startup fund. He is an affiliated professor with the chair for Computer Aided Medical Procedures (CAMP) at TU München, Germany, and full professor of image-guided therapies at the Otto-von-Guericke-University in Magdeburg, Germany. He is the listed inventor of more than 75 patent applications and the author of numerous papers. The following co-authors contributed to the article. All are or were affiliated with the chair of catheter technologies and image-guided therapies at the Otto-von-Guericke-University in Magdeburg, Germany: Juan Sanchez, MSc; Sathish Balakrishnan, MSc; Alfredo Illanes, Ph.D.; Axel Boese, Ph.D.; Yeshaswini Nagaraj, MSc; Robert Odenbach, MSc; Johannes Krug, Ph.D.; Michael Vogele, M.D.
The unparalleled soft tissue contrast and excellent image quality of MR have made it the imaging modality of choice especially for neuro and oncological applications.
The obtained MR images are then frequently used as relevant preoperative images for surgery planning, or as a visual reference directly in the surgery suite.
MR systems directly employed for therapeutic guidance or surgical monitoring are rarely available. The standard imaging systems in the surgery room are typically X-ray, ultrasound or endoscopy (video) performing the patient monitoring, controlling and device guiding functions.
Figure 1 (click image in upper right corner): Typical horizontal field 3T system with 70cm bore diameter. Actual therapy is difficult for the surgeon and only very little vertical space is available. A holding arm could be very helpful (shown in black), but must be very small and flexible to be of use.
To use these preoperative MR images also for therapy purposes usually requires fusion with the available imaging data in the surgery room. That is either not done, or happens only in the head of the clinician, so called cognitive fusion, or is accomplished by more or less accurate and complicated special software tools in combination with optical and/or electromagnetic device tracking systems.
For this fusion via software-based image co-registration the images are manually or semi-automatically registered to each other. A preoperative MR image, as the wording implies, was taken before the surgery, however, sometimes even on a bed with different curvature than the surgery table or in a different patient position.
For prostate MR, for example, the imaging is typically done with the patient in a straight supine position, while the actual biopsy or therapeutic treatment is performed prone or supine with the legs angled toward the torso. And for breast MR, the patient typically lies in an elevated prone position while surgery is performed on a surgical table in supine position or on the side. You easily recognize the difficulties using these preoperative MR images for accurate image fusion with the available imaging modalities available in the therapy or surgery room.
Real, precise registration is not possible that way with typical image registration errors in the order of 3-7mm, and in case of missing fiducial marker structures sometimes even significantly larger. That may be sufficient for actual therapies using an additional imaging system or for coarse orientation, but is too large for tissue biopsies and other precise therapies on small structures.
Using real time MR as a guidance device for intraoperative or interventional therapies (eg. biopsies and treatment of prostate cancer, liver laser-/radio-frequency-/ or cryo-ablations, brain interventions) could be very beneficial and would obviously eliminate or greatly reduce these registration errors.
This requires, however, that the therapeutic procedure is performed in the MR suite or the MR system is placed in a dedicated surgery room. The latter is an option that is explored by several institutions, but comes with very high investments and very highly skilled interdisciplinary staff.
Difficult patient access in conventional horizontal field superconductive magnets, and the need for special non-ferromagnetic therapy tools have also prevented a widespread occasional interventional use of conventional diagnostic MR systems. The interventional and therapeutic use of MR follows for the last 20-plus years the strategy to employ conventional standard high-field systems and add more or less complicated and expensive components.
MR-compatible robotic systems were, for example, proposed to solve the patient access issue in combination with specially shielded in-room monitors, dedicated nitinol or plastic devices with no or little susceptibility-related imaging artifacts, and in-room optical tracking systems. These components are quite expensive and the possible therapies are still limited because of the tight space in the MR bore and the issues around surgical sterility. The robotic systems are even needed with the short-bore magnets of the newest MR generation. With a magnet length of 1.2 meters it is still 60cm (an arms length) to the center of the magnet and with a bore diameter of 70cm, with a mid-size patient placed, there is only 10-15cm of available vertical space for a therapy tool (see figure 1).
Open vertical field magnets do provide some benefits for interventional procedures, but typically have only magnetic field strength of 0.2T to 0.4T with currently only one system over 1T. Lower field strength comes with increased acquisition times, which is not good for therapy applications, and a lower image quality. On the other hand, the lower field strength also reduces susceptibility artifacts and comes with a much lower magnetic attraction force, making the surgery generally safer.
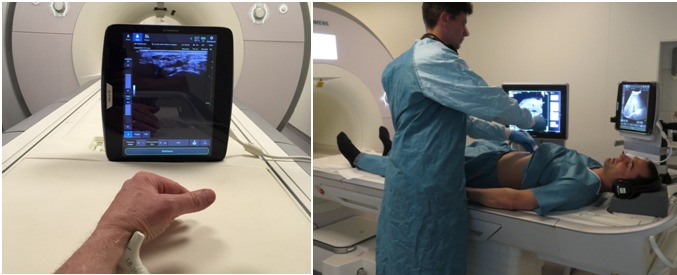
Figure 2: A tablet ultrasound of a large diagnostic imaging vendor placed only 1m away from the 3T MRI of another large imaging vendor. The ultrasound system is not approved and certified for use in the MRI suite, but direct applications under ultrasound guidance could give a new boost to performing interventional and therapeutic procedures in the MRI suite under ultrasound guidance. The picture on the right shows the cognitive fusion of MRI and US images on separate monitors.
So why not use the MR imaging capabilities and continue the procedure inside the imaging suite with an ultrasound system that is either cognitively fused (see figure 2) or automatically co-registered and overlaid to the just obtained MR images. Several commercially available ultrasound systems could theoretically be used even up to 1m to a 3T magnet opening (see figure 2). While these systems do not have an official MR safe label, research institutions have used these systems in phantom set-ups to rethink interventional MR procedures.
First, a comprehensive MR scan could be performed and the patient moved out of the magnet bore, but remaining on the MR bed. Live ultrasound images that are tracked using an optical inside-out approach adding a camera to the ultrasound probe in combination with an optical reference marker are then immediately fused with the MR images (see figure 3). This allows a comfortable US guided intervention and excellent patient access directly on the MR patient bed. This could then be combined with partly 3-D printed entirely mechanical MR compatible 7DOF holding arms keeping therapy devices and other tools in place (see figure 1). If additional MR imaging is required, the patient is moved back in the MR system. This set-up creates a very cost-efficient and effective environment that combines the advantages of MR and US by largely avoiding the drawbacks. And since most MR systems are almost exclusively used for diagnostic purposes, such an easy to set up and remove system would even be attractive for sites that only do few interventional or therapeutic MR procedures.
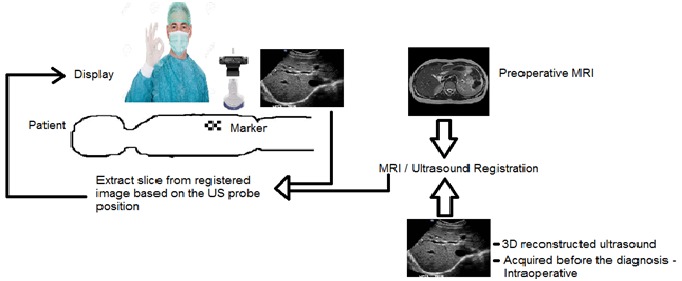
Figure 3: The concept of combining MR images directly with ultrasound inside the MR suite. For that, markers on the patient are used and a small camera system that is directly mounted to the ultrasound probe. The live ultrasound is then registered to the MR image and the actual procedure performed under ultrasound guidance. If additional MR imaging is required, then the patient is moved back into the magnet bore and subsequently the ultrasound registered again to the new image data set.
MR/ultrasound fusion is already offered by several vendors for prostate biopsy applications. With MR-compatible and approved ultrasound systems and easy-to-use and inexpensive accessories, interventional MR could become an attractive option again, also for other clinical applications.

Michael Friebe
About the author: About the author: Professor Michael Friebe, Ph.D., has been involved in diagnostic imaging and imageguided therapeutic products and services, as founder/ innovator/CEO, investor and scientist. Dr. Friebe is a board member of three startup R&D companies, as well as the investment partner of a medical technology startup fund. He is an affiliated professor with the chair for Computer Aided Medical Procedures (CAMP) at TU München, Germany, and full professor of image-guided therapies at the Otto-von-Guericke-University in Magdeburg, Germany. He is the listed inventor of more than 75 patent applications and the author of numerous papers. The following co-authors contributed to the article. All are or were affiliated with the chair of catheter technologies and image-guided therapies at the Otto-von-Guericke-University in Magdeburg, Germany: Juan Sanchez, MSc; Sathish Balakrishnan, MSc; Alfredo Illanes, Ph.D.; Axel Boese, Ph.D.; Yeshaswini Nagaraj, MSc; Robert Odenbach, MSc; Johannes Krug, Ph.D.; Michael Vogele, M.D.