
Katie Devlin
Preparing for the next wave of interoperability: Strategies for health plans
July 29, 2024
By Katie Devlin
Traditionally, payers have struggled to obtain clinical data in a structured format, which is crucial for determining appropriateness of treatment, utilization, and member engagement, and for capturing digital quality measures.
The 21st Century Cures Act established an ambitious vision for healthcare interoperability — the ability of two or more systems to exchange and use health information — but it wasn’t until recently that health plans had a clear path forward to achieve it, and to ultimately obtain the clinical data needed to support their strategic goals.
Now, the clock is ticking for payers to become compliant with the CMS Interoperability and Prior Authorization Final Rule. As payers prepare to meet these new requirements, which leverage industry best practices, they must create powerful partnerships and build an infrastructure to support interoperability at scale.
Forward-thinking health plans must ask themselves several critical questions as the state of healthcare interoperability continues to evolve.
Is your plan leaving data on the table?
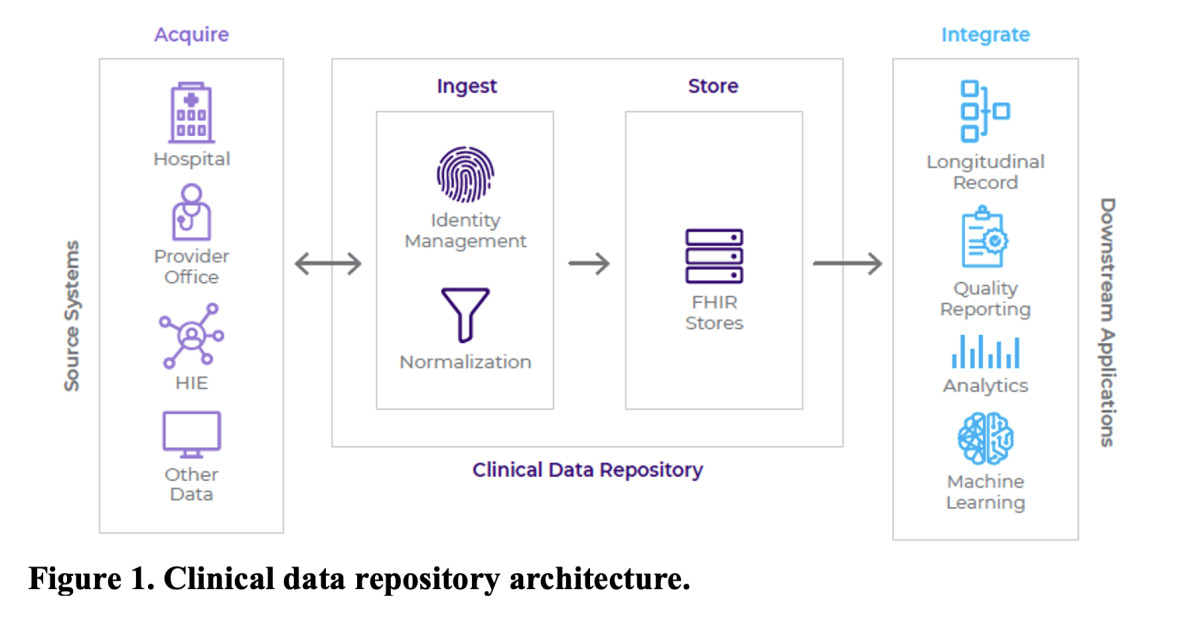
Payers rely on healthcare providers and other data sources to supply structured clinical information that they use for a range of applications, from Healthcare Effectiveness Data and Information Set (HEDIS®) reporting to population health management strategies. However, these partners aren’t all on a level playing field when it comes to interoperability — specifically regarding the use of FHIR.
The HL7® FHIR® (Fast Healthcare Interoperability Resources) standard has defined how electronic health records (EHRs) can be exchanged between payers and providers using application programming interfaces (APIs). When fully implemented, FHIR resources allow payers to share data more easily with downstream applications used for quality reporting, analytics and other aims.

At this time, FHIR is not frequently utilized for data sharing between payers and providers. Many providers prefer to send data via web-based portals or more traditional methods such as Integrating the Healthcare Enterprise (IHE) integration profiles. With this in mind, it’s important that payers remain agile and accommodate data partners where they are from a technical standpoint by offering FHIR APIs, IHE or web-based portals as connectivity options.
Is your plan ready for TEFCA?
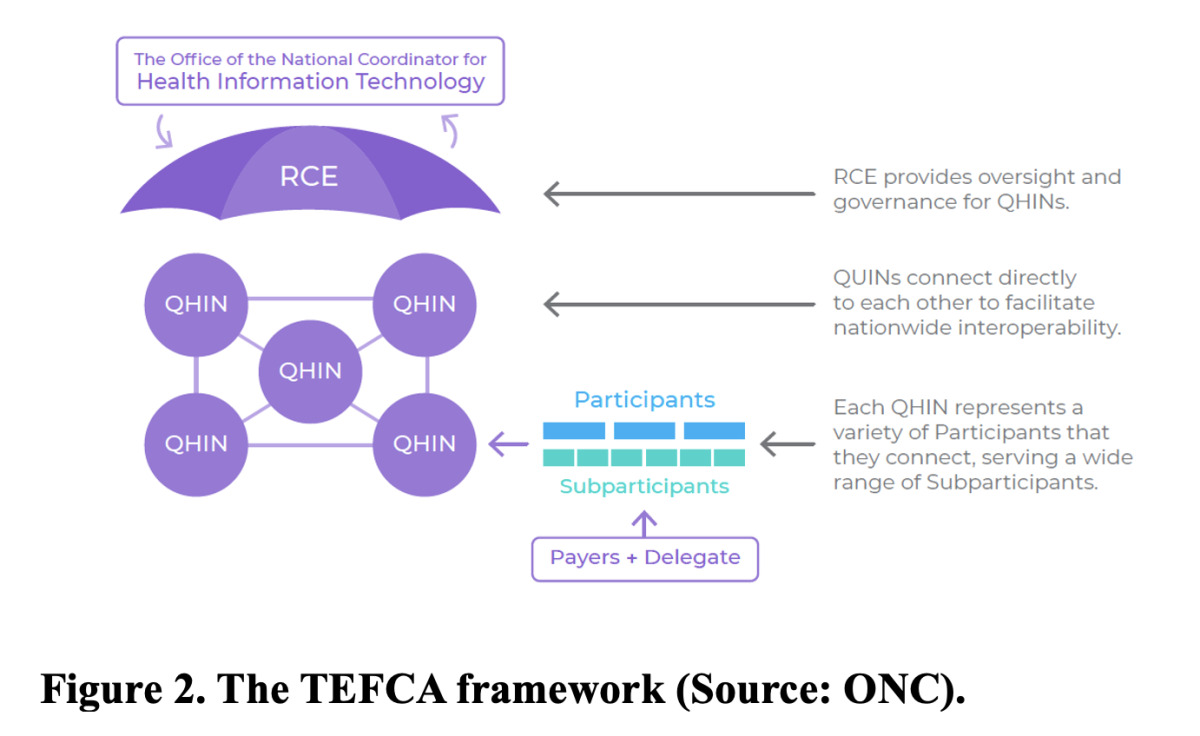
The Cures Act tasked the Office of the National Coordinator for Health Information Technology (ONC) with establishing a national framework for interoperability known as the Trusted Exchange Framework and Common Agreement (TEFCA). TEFCA provides a single on-ramp for healthcare stakeholders to exchange data, including payers. The Sequoia Project, which serves as the Recognized Coordinating Entity for TEFCA, released the second draft version of the Common Agreement in 2024, paving the way for broader data exchange.
Unlike the first version of the Common Agreement, which focused primarily on health information exchange for treatment and individual access, the latest iteration covers operational use cases relevant to payers, including uses related to quality improvement, risk adjustment and payment integrity. One of the most significant decisions for health plan leaders will be whether to join a qualified health information network (QHIN) and participate in TEFCA data exchange. A QHIN is a network of organizations (participants and sub-participants) that connect directly to each other to promote interoperability. To date, seven QHINs have completed the onboarding process to facilitate nationwide data exchange as outlined by TEFCA. These include KONZA National Network, eHealth Exchange, CommonWell Health Alliance, Health Gorilla, MedAllies, Epic Nexus and Kno2.

Health plans that opt to not join a QHIN may take advantage of TEFCA through a delegate partner. A delegate can handle the technical work to acquire data on behalf of any health plan listed in the Recognized Coordinating Entity (RCE) directory. This approach may be especially beneficial for small plans lacking the technical resources or expertise to manage the complex infrastructure needed for data exchange.
Will your plan make the 2027 API deadline?
Earlier this year, the Centers for Medicare & Medicaid Services (CMS) issued a final rule to improve communication around approvals and denials of prior authorizations (PAs) through data exchange practices. Payers are required to implement an API that can identify documentation requirements for a PA approval and communicate whether a payer approves or denies the request. Payers are also required to implement Provider Access APIs, to facilitate interoperability between payers and providers, as well as Payer-to-Payer APIs for data sharing across health plans.
These APIs must be implemented by January 1, 2027, requiring payers to move quickly and make the necessary infrastructure investments.
What other changes can payers expect?
Other industry developments affecting providers could deliver benefits for health plans. Specifically, recent changes targeting information blocking could help ease payer requests for medical records from providers.
In July 2023, the Department of Health and Human Services (HHS) Office of the Inspector General (OIG) released its final rule, which included a penalty that can reach up to $1 million for health IT developers and health information exchanges (HIEs) that unfairly restrict patient access to health information. However, this rule was limited in scope because it didn’t apply to provider organizations. According to the American Medical Association, providers that interfere with payers seeking electronic health information to confirm a clinical value are at high risk for information blocking.
To address this, a new rule has been proposed by HHS that would reduce reimbursement and impose other penalties on providers that block patient access to information.
Rapid progress toward interoperability
In the past, the healthcare industry had been somewhat reluctant to embrace opportunities to promote better data sharing. For example, when the Meaningful Use Program was first introduced back in 2009 to promote EHR adoption, the initiative took several years to gain traction. Now that the benefits for interoperability are clear, payers and other healthcare organizations will act quickly to join QHINs. Over the next 12 to 18 months, payers can expect to see more seamless data exchange between payers, health systems, HIEs and other organizations come to fruition.
How can payers get started?
Health plans looking to improve their interoperability strategy should first assess their infrastructure for scalability and compliance with interoperability standards. Furthermore, payers must collaborate with their legal, compliance, and subject matter experts to critically evaluate each potential data partner for compatibility with their market, infrastructure and use cases. Questions to ask include:
• Where does the partner have clinical data available for my use cases?
• What is the average patient match and document return rate for the partner?
• Do I need a Data Use Agreement?
• Where are my gaps from an infrastructure perspective? Do I have the ability to ingest data, standardize and normalize/enrich the information for downstream use cases, such as HEDIS reporting and year-round member engagement?
• What workstreams can be improved by leveraging this data across my organization?
With these considerations, payers will be able to access more structured clinical information for better decision-making. After years of hearing what’s possible through interoperability, health plans are finally positioned to realize the potential of data exchange to improve quality and close gaps in care.
About the author: Katie Devlin, DHSc, MS, CPHIMS, is vice president of interoperability for Cotiviti, a leader in data-driven healthcare solutions that enables healthcare organizations to deliver better care at lower cost through advanced technology and data analytics.
Traditionally, payers have struggled to obtain clinical data in a structured format, which is crucial for determining appropriateness of treatment, utilization, and member engagement, and for capturing digital quality measures.
The 21st Century Cures Act established an ambitious vision for healthcare interoperability — the ability of two or more systems to exchange and use health information — but it wasn’t until recently that health plans had a clear path forward to achieve it, and to ultimately obtain the clinical data needed to support their strategic goals.
Now, the clock is ticking for payers to become compliant with the CMS Interoperability and Prior Authorization Final Rule. As payers prepare to meet these new requirements, which leverage industry best practices, they must create powerful partnerships and build an infrastructure to support interoperability at scale.
Forward-thinking health plans must ask themselves several critical questions as the state of healthcare interoperability continues to evolve.
Is your plan leaving data on the table?
Payers rely on healthcare providers and other data sources to supply structured clinical information that they use for a range of applications, from Healthcare Effectiveness Data and Information Set (HEDIS®) reporting to population health management strategies. However, these partners aren’t all on a level playing field when it comes to interoperability — specifically regarding the use of FHIR.
The HL7® FHIR® (Fast Healthcare Interoperability Resources) standard has defined how electronic health records (EHRs) can be exchanged between payers and providers using application programming interfaces (APIs). When fully implemented, FHIR resources allow payers to share data more easily with downstream applications used for quality reporting, analytics and other aims.
At this time, FHIR is not frequently utilized for data sharing between payers and providers. Many providers prefer to send data via web-based portals or more traditional methods such as Integrating the Healthcare Enterprise (IHE) integration profiles. With this in mind, it’s important that payers remain agile and accommodate data partners where they are from a technical standpoint by offering FHIR APIs, IHE or web-based portals as connectivity options.
Is your plan ready for TEFCA?
The Cures Act tasked the Office of the National Coordinator for Health Information Technology (ONC) with establishing a national framework for interoperability known as the Trusted Exchange Framework and Common Agreement (TEFCA). TEFCA provides a single on-ramp for healthcare stakeholders to exchange data, including payers. The Sequoia Project, which serves as the Recognized Coordinating Entity for TEFCA, released the second draft version of the Common Agreement in 2024, paving the way for broader data exchange.
Unlike the first version of the Common Agreement, which focused primarily on health information exchange for treatment and individual access, the latest iteration covers operational use cases relevant to payers, including uses related to quality improvement, risk adjustment and payment integrity. One of the most significant decisions for health plan leaders will be whether to join a qualified health information network (QHIN) and participate in TEFCA data exchange. A QHIN is a network of organizations (participants and sub-participants) that connect directly to each other to promote interoperability. To date, seven QHINs have completed the onboarding process to facilitate nationwide data exchange as outlined by TEFCA. These include KONZA National Network, eHealth Exchange, CommonWell Health Alliance, Health Gorilla, MedAllies, Epic Nexus and Kno2.
Health plans that opt to not join a QHIN may take advantage of TEFCA through a delegate partner. A delegate can handle the technical work to acquire data on behalf of any health plan listed in the Recognized Coordinating Entity (RCE) directory. This approach may be especially beneficial for small plans lacking the technical resources or expertise to manage the complex infrastructure needed for data exchange.
Will your plan make the 2027 API deadline?
Earlier this year, the Centers for Medicare & Medicaid Services (CMS) issued a final rule to improve communication around approvals and denials of prior authorizations (PAs) through data exchange practices. Payers are required to implement an API that can identify documentation requirements for a PA approval and communicate whether a payer approves or denies the request. Payers are also required to implement Provider Access APIs, to facilitate interoperability between payers and providers, as well as Payer-to-Payer APIs for data sharing across health plans.
These APIs must be implemented by January 1, 2027, requiring payers to move quickly and make the necessary infrastructure investments.
What other changes can payers expect?
Other industry developments affecting providers could deliver benefits for health plans. Specifically, recent changes targeting information blocking could help ease payer requests for medical records from providers.
In July 2023, the Department of Health and Human Services (HHS) Office of the Inspector General (OIG) released its final rule, which included a penalty that can reach up to $1 million for health IT developers and health information exchanges (HIEs) that unfairly restrict patient access to health information. However, this rule was limited in scope because it didn’t apply to provider organizations. According to the American Medical Association, providers that interfere with payers seeking electronic health information to confirm a clinical value are at high risk for information blocking.
To address this, a new rule has been proposed by HHS that would reduce reimbursement and impose other penalties on providers that block patient access to information.
Rapid progress toward interoperability
In the past, the healthcare industry had been somewhat reluctant to embrace opportunities to promote better data sharing. For example, when the Meaningful Use Program was first introduced back in 2009 to promote EHR adoption, the initiative took several years to gain traction. Now that the benefits for interoperability are clear, payers and other healthcare organizations will act quickly to join QHINs. Over the next 12 to 18 months, payers can expect to see more seamless data exchange between payers, health systems, HIEs and other organizations come to fruition.
How can payers get started?
Health plans looking to improve their interoperability strategy should first assess their infrastructure for scalability and compliance with interoperability standards. Furthermore, payers must collaborate with their legal, compliance, and subject matter experts to critically evaluate each potential data partner for compatibility with their market, infrastructure and use cases. Questions to ask include:
• Where does the partner have clinical data available for my use cases?
• What is the average patient match and document return rate for the partner?
• Do I need a Data Use Agreement?
• Where are my gaps from an infrastructure perspective? Do I have the ability to ingest data, standardize and normalize/enrich the information for downstream use cases, such as HEDIS reporting and year-round member engagement?
• What workstreams can be improved by leveraging this data across my organization?
With these considerations, payers will be able to access more structured clinical information for better decision-making. After years of hearing what’s possible through interoperability, health plans are finally positioned to realize the potential of data exchange to improve quality and close gaps in care.
About the author: Katie Devlin, DHSc, MS, CPHIMS, is vice president of interoperability for Cotiviti, a leader in data-driven healthcare solutions that enables healthcare organizations to deliver better care at lower cost through advanced technology and data analytics.