Protons have been in use in medicine for nigh on 50 years, but modern proton therapy can hardly be considered mainstream. Many in the field of radiology oncology consider proton therapy to be one of the most advanced medical treatments available, but providing access is no easy matter. Opening a major proton center involves laying down more than $100 million in construction costs and a technological investment that takes up a city block and many tons of concrete to support it. It is no wonder that there are only seven proton centers in operation in the United States, but that number is projected to grow steadily in a matter of a few years. Several more large-scale centers are set to open their doors within five years' time, and an increasing number of lower-cost and smaller-scale proton therapy technologies are preparing for launch, which might alter the trajectory of this very high-tech industry.
Proton therapy is similar in concept to any other form of external beam radiation therapy-the idea is still to target and kill tumor cells by disrupting their haywire DNA, but proton beams have properties that make them ideal for cancer therapy. In short, more of the radiation dose is delivered to the targeted site, thereby sparing more of the healthy tissue that would otherwise be down for the count with conventional radiation therapies using X-ray technology.
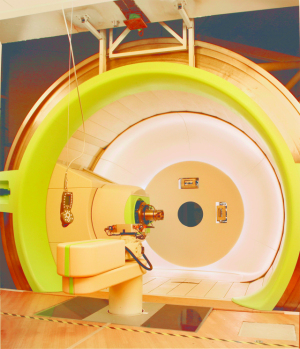
A patient being
prepared for proton
therapy at the
M.D. Anderson Cancer
Center.
There is also less concern about patients developing secondary cancers as a result of radiation treatment. With better so-called dose conformity, oncologists could even seek to increase the dose to provide stronger, more effective proton therapy in fewer treatments. The only real drawback is the cost of building and maintaining one of these centers, which filters into treatment cost and the overall cost of cancer treatment.
Picturing proton therapy
To get a glimpse of proton therapy technology in action, DOTmed visited M.D. Anderson's Proton Therapy Center in Houston and took a tour of the facility with medical director Dr. Andrew Lee. One gantry is set up with state-of-the-art pencil-beam scanning capabilities and an eye chair. Other treatment rooms house a fixed beam line and an experimental beam line, and accompanying all of this is a dedicated machine shop set-up to create plastic compensators and brass apertures that custom sculpt the beam and the subsequent radiation dose for each patient. At full capacity, M.D. Anderson's center can treat 3,500 patients annually and employs about 85 physicians, physicists, dosimetrists, technologists and other staff.
The M.D. Anderson Center uses a synchrotron instead of a cyclotron to accelerate the proton particles in preparation for therapy. The synchrotron produces discrete energies, whereas cyclotrons put out a high-energy beam that is then degraded if a lower-energy beam is needed for treatment.
It all starts with a tank of hydrogen about the size of a fire extinguisher, which is then oscillated. The protons that split off are then accelerated to about two-thirds the speed of light inside the synchrotron. By the end of acceleration, the particles have traveled enough distance to equal 12 or 13 flights in orbit around the earth's equator. The beam is then directed to one of the treatment rooms, three of which house the massive 360-degree rotating gantries that run 13 meters in diameter and weigh about 190 tons, or, as Dr. Lee explains, the weight of a jet airliner without passengers. Standing behind the scenes on a narrow catwalk overlooking a massive, two-story masterpiece of engineering surrounded by miles of wires as it rotates to sub-millimeter precision, it is easy to see what all the excitement is about. For the people involved, the concern is not so much about the cost, but the exploration of the technology and developing the best possible cancer treatment for patients. One aspect somewhat hobbling the technology is the paucity of clinical studies conducted to confirm proton therapy's superiority over conventional X-ray therapy, and results to some studies have been unclear on this point.
Stephen Hahn, MD,
and James Metz, MD.
Is it really better?
With that said, it should be noted that a recent study conducted by Harvard Medical School and Massachusetts General Hospital in Boston found a 50 percent drop in secondary cancers for patients who were treated with proton therapy compared with X-ray therapy. Other studies have shown definitive advantages in treatment for pediatric and ocular cancers and chordomas at the base of the skull.
Applications for lung cancer are also at the cutting edge of proton therapy. The M.D. Anderson Proton Therapy Center is renowned for its treatment of lung cancer. Proton therapy's benefit over conventional radiation therapy for prostate cancer has not yet been proven, but some in the industry swear that proton therapy means fewer complications and secondary malignancies, making it an important choice in prostate cancer treatment planning.
Protons for pediatrics
Perhaps the greatest application for proton therapy is in pediatric medicine, a field hyper-sensitive to the issue of radiation dose and the after-effects of treatment.
"For kids, one of the things about radiation therapy is that even low doses can have pretty profound effects later in life," says Dr. Lee. "That can be as obvious as cosmetic defects, because if bone is exposed to a certain dose of radiation in a growing child, it's not going to grow at the same rate as bone that isn't exposed. It could be something in between, like cognitive defects - maybe they have a little bit of trouble paying attention in school. It could be something really subtle."



Ad Statistics
Times Displayed: 133880
Times Visited: 7662 MIT labs, experts in Multi-Vendor component level repair of: MRI Coils, RF amplifiers, Gradient Amplifiers Contrast Media Injectors. System repairs, sub-assembly repairs, component level repairs, refurbish/calibrate. info@mitlabsusa.com/+1 (305) 470-8013
The other end of the spectrum of complications is far more serious. Radiation exposure to the lungs and heart at a young age can spell subsequent tumors later.
"The more tissue that is exposed to radiation, the higher the chance that that patient may develop a secondary radiation-associated malignancy later in life," says Dr. Lee. "It seems that children are more sensitive to it than patients who are much older, so we want to minimize the exposure as much as possible."
Dr. Lee also noted a recent study in the Journal of Clinical Oncology that stated a correlation between radiation doses as minimal as 5 Gy of radiation, which isn't even considered therapeutic, and a clear increase in cardiac mortality.
The newest proton center, Penn Medicine's Roberts Proton Center in Philadelphia, is partnering with the Children's Hospital of Philadelphia and will be dedicating an entire treatment room just for pediatric cases. Similar partnerships are also underway at other centers.
Building demand for proton therapy
According to a recent market research report on proton therapy centers in the U.S., there has been a 200 percent jump in the number of prospective sites and 75 percent overall growth in the number of centers online or being commissioned from 2005 to 2010. The report also noted that demand for small-scale facilities might overtake large-scale facilities in time.
The National Association for Proton Therapy (NAPT) was founded in 1990 at the same time as the opening of the first clinically-based center - the James E. Slater, M.D. Proton Treatment and Research Center at Loma Linda University Medical Center in California. Since then, NAPT has served as a resource center for patients, physicians and developers of centers. Its leadership keeps track of all sites under construction and in development. Executive Director Leonard Arzt is also in the know about the various technologies in the pipeline and the challenges that proton therapy faces in today's daunting political and economic climate.
"I think one of the major challenges is to produce more clinical studies, but our centers are in the midst of doing that," says Arzt. "The challenge is also not having enough treatment slots or rooms for all the patients who want to be treated with proton therapy. I would say that there is no shortage of patients or demand for proton therapy. There are challenges, not for our current operating centers that are doing quite well, but for those who want to build proton centers and find funding to get one off the ground, but there is no shortage of interest."
It's true that there is a great deal of uncertainty and risk involved in developing proton centers as funding has become increasingly scarce, whether from grants, loans or private capital, and there is some question about how Medicare reimbursement rates will be set in the near-term, which will affect private payer rates in the long-term. In 2008 and 2009, there were double-digit decreases in the Medicare reimbursement percentages for proton therapy. This year, there is a 34 percent increase in reimbursement, which has the whole market looking on with uncertainty as to the future of payer behavior.
Regardless of the risks, there is still plenty of demand for proton therapy. Dr. Lee estimates that patient populations in need call for something around 200 treatment rooms. It's an understatement to say that there's some disparity when there are currently only about 23 operating proton treatment rooms in the world in contrast with the number of conventional linear accelerator rooms - which rounds out to about 10,000.
"I think that at this point in the game of radiation therapy, proton therapy is about as small as one can get," says Arzt. "Proton therapy represents a miniscule slice of the total radiation therapy treatment pie. In fact, proton therapy is at this point less than 1 percent of all external beam radiation therapy treatments."
Still, the number of those treated with proton therapy is rising steadily. The Roberts Proton Therapy Center in Philadelphia is the latest in brand new proton centers. Patients are now being treated at the facility, which features a 75,000 square-foot facility with a cyclotron and four treatment rooms at a cost of about $140 million. As if all this doesn't seem futuristic and space-aged enough, the Roberts Center in Philadelphia has partnered with NASA to test the effects of cosmic radiation on astronauts during long-term space travel.
The remaining four operating proton therapy centers in the U.S. are the Francis H. Burr Proton Center at Massachusetts General Hospital in Boston; the Midwest Proton Radiotherapy Institute at Indiana University in Bloomington; the University of Florida Proton Therapy Institute in Jacksonville and the Oklahoma City Proton Therapy Center.
New Facilities Forecast
The Roberts Center may be the newest, but a handful of centers are poised to steal the title. Other centers that have broken ground include the Hampton University Proton Therapy Institute in Hampton, Va, the North Illinois University Proton Therapy Center just outside Chicago and ProCure's CDH Proton Therapy Center based in Warrenville, Ill., which is scheduled to open in 2011.
The beam transport
system distributes a
beam of proton
energy to each
of the four
treament rooms quickly
and efficiently.
Photo courtesy of
ProCure Treatment Centers, Inc.
ProCure is a private health care provider and developer of proton centers headquartered in Oklahoma City. The organization was responsible for the recent opening of the Oklahoma City Proton Center in the fall of 2009, and about 60 patients have completed fractionated treatments there. ProCure CEO Hadley Ford told us construction is now underway for a new Somerset, N.J, center that is scheduled to open for treatment in about two years. Ford says developing a proton therapy center involves a plethora of considerations and potential pitfalls along the way.
"It is a phenomenally complicated process precisely because it is a very recent industry," says Ford. "There's only a handful of proton centers around the world and there is an incredible amount of competencies that one needs to make this happen - from building design to construction, to training, finance, legal structures and partnering protocols for treatment. The list goes on and on."
Development for future centers is in the works for south Florida, other parts of California, and in Seattle at the Seattle Cancer Care Alliance. Midtown Manhattan is supposedly getting a $200 million, 200,000 square-foot facility sometime in 2011 dubbed the Proton Institute of New York - a collaboration between major NYC cancer hospitals. In other parts of the world, proton therapy is already available or in development in Japan, Germany, France and Switzerland.
On a smaller scale
There are a handful of manufacturers focusing on building smaller and lower-cost, single-vault concepts for proton therapy and at least two new technology platforms are in development. Two of these manufacturers are Still River Systems and Compact Particle Acceleration Corporation (CPAC).
"The technology is yet to be proven or installed anywhere, but that could certainly be a game-changer and may alter the proton therapy landscape if and when there are enough of them up and running in the hospitals they have agreements with," says Arzt.
Still River Systems already has about 12 or so tentative agreements set up for its smaller footprint superconducting cyclotron technology, Dr. Lionel Bouchet, physicist and director of Still River Systems, explains.
"This is all about scaling down the size of the proton generators and by 'scaling down' we mean the order of magnitude," says Dr. Bouchet. "We reduce the cost by reducing the global size of proton therapy."
The concept behind Still River Systems' technology was developed in the early 2000s and is based on technology borrowed from the MR industry using a very powerful, but much smaller, cyclotron that has the superconductive power of a research-strength MRI unit.
Graphic of a
compact proton therapy
system being developed
by the Compact
Particle Acceleration Corp.
The system is
the only one
capable of fitting
inside a conventional
radiotherapy suite.
"We have a 9 Tesla cyclotron, which is two to three times more powerful than a commercial MRI, and the total weight is about 20 tons compared to the 220 tons of the cyclotrons used for more conventional proton therapy," says Dr. Bouchet.
Washington University in St. Louis, Mo., is preparing to be the first to install a single-vault proton therapy system, and Still River Systems has two other sites under construction, one at the Robert Wood Johnson University Hospital in New Jersey, and another at the University of Oklahoma Cancer Institute in Oklahoma City.
"Each room is fully independent compared to the typical proton center where you have one proton source and multiple gantries," says Dr. Bouchet. "When you are dependent on one proton source that feeds into multiple rooms there is less reliability, because if anything goes wrong with the cyclotron, the whole facility goes down. The clinical aspect is the same; it's more of the practical aspect."
Dr. Jeffrey Bradley is director of the S. Lee Kling Center for Proton Therapy of the Siteman Cancer Center at Washington University, where the first Still River Systems proton therapy unit is being installed. Dr. Bradley says the decision to go with Still River Systems had a lot to do with cost.
"It's about a quarter of the cost of a multi-room treatment system," says Dr. Bradley. "That's the advantage of a smaller-scale unit, and this is the first smaller-scale type proton unit that will be commercially available."
Once up and running, Dr. Bradley estimates that the center will be treating a minimum of 25 patients daily with proton therapy, thereby improving upon the treatment offered to the thousands of patients who seek treatment at the Siteman Center every year.
"I think as the experience and expertise increases with proton therapy, the types of cancers and the types of patients that are treated will increase," says Dr. Bradley. "The growth of proton therapy has been slow because of the cost of installing these facilities and that is what has held up the number of slots for patients."
Going linear
Another proton platform in development uses something called a dielectric-wall accelerator. DOTmed spoke with Shawn Guse, CEO of CPAC, about the technology originally designed for defense-related research at Lawrence Livermore National Laboratory, and now being co-developed by CPAC and TomoTherapy to devise an even smaller-scale proton therapy system. Guse says their system is much more of a classical linear accelerator in that developers haven't sought to bend the trajectory of the particles during acceleration.
"From a clinical perspective, the most important thing for us is the ability to control the beam electrically within the accelerator," says Guse. "Rather than accelerate the particle up to a maximum energy and then attempt to manipulate it, as conventional cyclotrons and synchrotrons typically do, we simply only accelerate the particle up to the energy that is needed for that particular pulse of protons."
Guse says synchrotrons have more control over the energy of the beam, but that dielectric-wall accelerators take it a step further by being able to vary the energy of the beam to a greater degree. CPAC's design involves an accelerator that is well under a ton, which means far less mechanical stress and a much smaller device. The company is currently working with a subscale accelerator and there are hopes of having a full-scale model ready in approximately three years' time.
"The model that we're faced with today is to have two to five treatment rooms to make the center economically viable," says Guse. "With the ability to install a system in a single room at a per-room price that is at or below what you could do with a multi-room center, that is much more aligned with the way hospitals adopt other technologies."
On the flip side, Ford says he studies all the equipment soon to be available for ProCure's proton centers, but the large-scale facility still makes more sense.
"The equipment cost [for a large-scale center] is really about $15 or $16 million per room," says Ford. "We look at some of these single-room solutions and the equipment cost is actually the same or higher than the equipment cost we're paying already. The difference is that they are bundling it differently. It's like, 'Do I want to buy a liter container of Coke or the six-pack?' The six-pack, theoretically, is cheaper because you can buy one can, but on a volume basis you're actually paying more."
Pushing down the cost
The first proton centers had no market or cost point of reference, but industry leaders say as more and more centers open, competition and experience will force the price down to something a little more manageable.
"The cost will definitely go down and it's already going down," says Arzt. "Loma Linda had a clean canvas. The technology was not off-the-shelf and they created the foundation for building proton centers and it was a trial-and-error situation. I would say the cost will come down for multi-room centers but they are still up there at $100 to $125 million for full-scale proton centers with three or four gantries and one or two fixed beams."
For those who might look upon proton therapy as an exorbitantly expensive medical treatment, Arzt says proton therapy doesn't even make a blip on the radar screen of total health care costs. "We're all for reducing health care costs - proton therapy has not and will not impact that."
The future of proton therapy
Proton therapy may represent less than 1 percent of all external beam radiation treatments, but market research projects that there will be an almost 200 percent growth in the number of patients receiving proton therapy in the next five years.
Ford says that by that time, more focus will be on sparing healthy tissue, regardless of the extra cost, and more studies should show a clearer picture of the long-term effects of radiation therapy on those healthy tissues.
"If you and I were both unfortunate enough to have a brain tumor, and I was treated with this state-of-the-art X-ray technology called IMRT and you were treated with protons, I would get a whole bunch of extra radiation in my brain that you didn't get," says Ford. "Now the question is, well, is that a good thing or a bad thing? It's never going to be a good thing. The question is, how bad is it? It's perfectly possible that nothing will happen, but the brain is a very sensitive area for radiation. However, let's look at the amount of radiation that I received. You can look at all the fancy dose washes and treatment plans, but ultimately the amount of extra radiation that I received because I got X-rays and you got protons is equivalent to between 100,000 and 400,000 dental X-rays without that lead shield protecting you."
Guse believes that proton therapy ranges widely in quality and may be in the midst of a slow metamorphosis from the use of passive scattering beams and the more advanced scanning beams, to the motherlode of proton therapy-proton IMRT.
"I put the standard of quality on three levels," says Guse. "The first is the standard proton therapy beam, where the beam is spread out and shaped by external devices. The next step is the spot or pencil-scanning beam, where a small pencil beam is moved back and forth across the target area to fill in the dose required for the tumor. The third and highest quality would be an intensity modulated proton therapy beam that is able to adjust the intensity of the beam for each pulse that is delivered. If you can take that and marry it with a scanning device, you'll get the best of all worlds."
The only facility that currently has this technology, says Guse, is the Paul Sheer Institute just outside Zurich. CPAC's new proton device will hypothetically have these capabilities.
Slow, steady growth
The key obstacles for proton therapy are the cost of building and maintaining these centers and the lack of clinical proof showing the efficacy of proton therapy compared with conventional therapies. This is expected to begin changing within a few years.
"Over the next five years, there will be an inflection point where more and more studies will come out that make it glaringly obvious that it's really the standard of care - and that if you are going to have a serious cancer center, you need to have access to proton therapy," says Ford.
The future is bright, but proton therapy won't be appearing in every major hospital and cancer center overnight.
"These centers are very big and complex," says Ford. "They aren't going to spring up on every corner like an MRI. This is going to be an industry that will develop very rationally and slowly over time."